|
New innovations in orthopedic surgery continue, but nowhere as quickly as shoulder arthroplasty. In the last 2-3 years, the FDA has cleared the first canal sparing, sometimes called the stemless shoulder replacement, the Wright/Tornier Simpliciti shoulder arthoplasty system. This company has also been responsible for the development of augmented glenoids (shoulder sockets) for defects and problems that had previously been very difficult to reconstruct. Finally, Wright/Tornier along with the software company, Imascap, developed a software program based on CT scans for surgical preplanning and intraoperative guidance. As a conservative surgeon, I was not one of the first adopters of the canal sparing design. I wanted to see results and proof before using this technology on my patients. That proof came from some of the best shoulder replacement surgeons in the country and the world, and I was convinced. It took less prodding to start using the Blueprint planning software. I attended the Tornier Masters course about two years ago in Minnesota and had several lectures touting this technology. It makes good sense that going in with a plan is better than having no plan at all. The fate was sealed after speaking with Gilles Walch, a world renowned French shoulder specialist. I admire the French for a couple of things in particular, bordeaux wines and advancements in shoulder surgery. He is legendary in France. At my home, we jokingly refer to Dr. Walch as a shoulder surgery god! He developed the Blueprint software but said that even if he had not, he would use it in every single case. My decision was made. If a "shoulder god" could be a better surgeon with this technology, my patients and I would benefit even more.  These two pieces of metal and the software that was used to create them can make your surgeon 10 times more accurate. Who wouldn't want that? Those surgeons that use preplanning are likely to be more accurate even without the 3D printed guides than those who do no preplanning.  The larger chunk on the left is a 3D metal printing of the socket and the smaller piece on the left is the guide that fits to the glenoid in surgery to place the guide pin in the correct position and angle. With this, the guide pin variance in position is less than 1 mm and the angle variance in any direction is approximately 1 degree versus 10-11 degrees without the guide.  I get my hands on the glenoid before I ever cut the skin. Yes, that is my thumb. For those wondering, it is brachydactyl type D, a common thumb difference affecting a small percentage of the population. Nevertheless, I get to feel and experience the defects of the socket before surgery. The second smaller hole on the guide is an antirotation drill hole. It is designed for use with augmented glenosphere to ream the portion of the socket that needs to be augmented. This patient had 25 degrees of tilt of his glenoid, 0-8 degrees is normal. If this isn't corrected, the shoulder replacement will fail much more quickly. 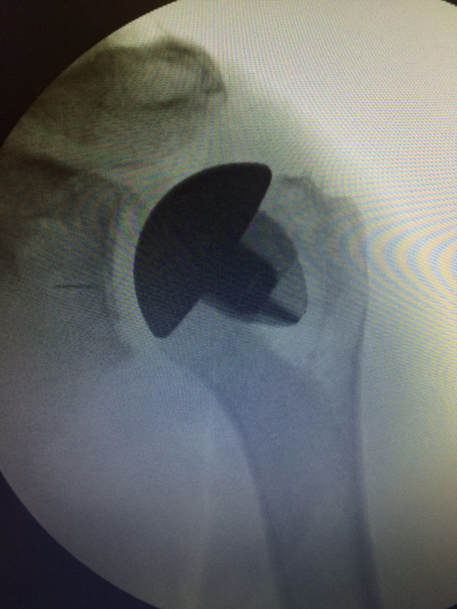 This xray is the culmination of all three technologies and in my opinion the very best that I or anyone else could have offered the patient. We were able to anatomically restore the shoulder alignment with thorough planning and new augmented socket designs and use a canal sparing implant which in my experience has resulted in less pain postoperatively for the patient.
My goal for all of my patients is to do the best, most conservative treatment. If that is surgery, I will use all the best new innovations at my disposal to perform the best, longest lasting surgery possible.
0 Comments
Leave a Reply. |
AuthorOrthopedic Shoulder and Elbow Surgeon back in his hometown to practice Archives
August 2022
Categories |
 RSS Feed
RSS Feed